
In From Killer to Common Cold Dr. David Graham takes an investigative approach to track down this new serial killer. Of course the killer in question is SARS-coV-2, the villain in the first modern-day pandemic. The virus leads to the sickness known as COVID-19. Dr. Graham suggests that within 2 to 5 years SARS-coV-2 will become another common cold. That is the destiny of this coronavirus. And that destiny is already written. How does the pandemic end? Read on.
There is no such thing as ‘herd immunity’. We must strive for herd protection.
Three ingredients for a pandemic.
An infectious agent needs three conditions to cause a pandemic.
- It needs to cause disease in humans
- It needs to be highly transmissible
- Humans have no pre-existing immunity to it
Unfortunately, the virus has already killed over 1,000,000 people by October 2020, and the virus checks all of those boxes.
The following is selected and at times edited excerpts – From Killer to Common Cold.

The destiny is written.
I believe that the destiny of SARS-CoV-2 is already written. With or without a vaccine, with or without an effective treatment, with or without expected technological advances, we are destined to interact with this virus forever. SARS-CoV-2 is not eradicable and will become endemic.
There are already four coronaviruses that are endemic and cause the common cold. SARS-CoV-2 will become the fifth endemic human coronavirus. The virus that causes COVID-19 will become another common cold.
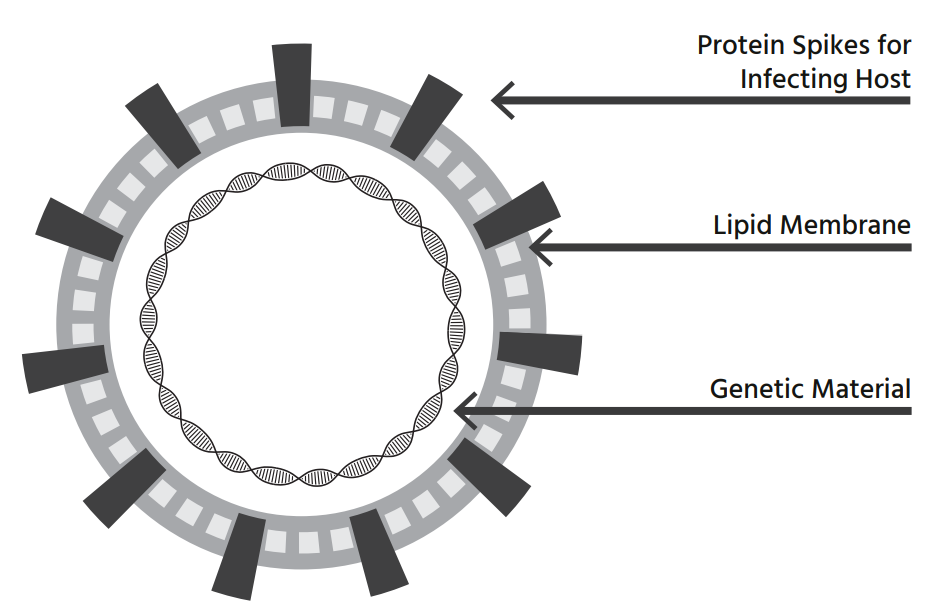
Virus 101.
A virus is not alive. It only comes to life when it enters your body. Once it gets inside your body, it attaches to cells and it simply wants to make copies. In the end, replication is what all lifeforms “want.”
Our bodies will try and fight the intruder with antibodies. To simplify, there are different T-cells that orchestrate your cellular immune system. Some T-cells detect your cells that are infected and kill them, stopping the production. But these anti-coronavirus antibodies wane over time and may or may not protect you from future infection.
A virus wants to be benign, because usually that is the best mechanism to replicate and spread. That may help our cause, in the end.
In the survival of the fittest, the fittest Covid-19 virus is the one that makes the most copies of itself. Certainly, we will see genetic changes in SARS-CoV-2 that affect its ability to replicate.
Evolutionary biology can help humans and SARS-CoV-2 both reach our goals. Through behavioral modifications, humans can suffer and die less from infection, and SARS-CoV-2 can evolve to reproduce itself more. Believe it or not, as a novel host to SARS-CoV-2, humans need to help, rather than hinder SARS-CoV-2 to reach its goal. A benign virus is a good virus.
The common flu.
Influenza is one of the greatest viruses of all time in terms of its ability to escape the immune system. There is no other respiratory virus in its class. Every year, influenza changes a little. With minor mutations. Generally, 20-50% efficacy is expected from seasonal influenza vaccination.
The problem with a coronavirus is that immunity to it is not long lasting. In 6-24 months, despite having a perfectly adequate initial immune response, you might get the same virus again as your immunity wanes.
More often than not, the elderly struggle to produce antibodies to influenza after vaccination. Thus, those at highest risk for complications from influenza are often the least protected by vaccination. With Covid-19, this is also the concern. Those most at risk for Covid-19—the elderly and immunocompromised—simply won’t respond to Covid-19 vaccines, either.
Despite concerns about effectiveness, if you get a vaccine for Covid-19, you might still get the virus, but hopefully you will be less sick.
Herd protection, not herd immunity.
Instead of herd immunity, we need to pay attention to herd protection. Herd protection is the threshold past which we break the back of epidemic transmission. Once herd protection is reached, regional communities stop having regional epidemics.
Herd protection is affected by the number of people who get the disease, who get vaccinated, who have pre-existing immunity, and who are excluded by heterogeneous mixing of the population. It stops the epidemic transmission for now. It doesn’t eradicate the disease.
Fighting COVID-19 with the common cold, and more.
There remains an unexplained phenomenon regarding why young children don’t frequently get sick from endemic coronaviruses. That is the power of pre-existing immunity, where your memory T-cells remember that you have had this virus before (or a similar version), and immediately get back to work controlling the virus. Common cold immunity can fight SARS-coV-2. In fact, somewhere between 20-50% of people have cross reactive T-cells present prior to any SARS-CoV-2 exposures.
SARS-coV-2 some folks just don’t get it.
Even without pre-existing immunity from prior exposure to common cold coronaviruses, it seems that a segment of folks do not get Covid-19 after exposure. That is, perhaps there are some people who are not susceptible to Covid-19 infection. They simply don’t get it.
The percentage of the population at risk certainly isn’t 100%. We know this, because not everyone in a house tests positive after close family exposure. For instance, in a close-knit family, sometimes only 50% of family members ever test positive. We saw the same event on cruise ships. There are rare folks who lack the cellular receptors.
The virus lacks the ability to attach to their cells.
This event along with the pre-existing immunity (from previous common colds) lowers the herd protection threshold.
How we humans mix is also in the mix.
I want to specifically mention heterogeneous mixing of populations, as there are folks who are going to get Covid-19 and those who are less likely to get it. We don’t mix randomly, but rather with the same people over and over again. And some mix more than others. When we adjust for our mixing behaviour, the herd protection threshold goes down even more.
Thus, heterogeneous mixing of the population lowers the attack rate but is not taken into account in most models of Covid-19 herd immunity. Social butterflies will become, at the very least, partially immune. Those who continue to isolate at home won’t get Covid-19, which lowers the herd protection calculation.
Vaccines will help the cause, but they’re not a cure.
With Covid-19, since immunity is neither long lasting nor complete, vaccination will not lead to local elimination or eradication. Even if we have effective vaccinations against SARS-CoV-2, we know immunity will wane and Covid-19 will continue to circulate regionally. With or without a vaccine, Covid-19 will cause human disease indefinitely.
None of the other human coronaviruses provoke permanent immunity, even after natural infection. Immunity is temporary, and just like common cold coronaviruses, re-infection is expected after a period of time. This is true after natural infection and likely will be true after immunization as well.
Our immune system also plays a role in modifying the severity of disease. That is, once you have had an infection once, the second time may not be as bad as the first. The third time it might be the common cold. Through vaccination or prior infection, you prime the immune system so that it recognizes the virus and ramps up more quickly. Vaccines may affect how long the transitional period lasts. Vaccines sow some amount of immunity into the population and may actually shorten the time to reaching herd protection.
When does the pandemic end?
There is no specific event or number that signifies the beginning or the end of the Transitional Phase. There won’t be trumpets or an announcement to tell you that your community has reached it. The transition will be gradual. One can imagine significant community vaccination as a possible precipitating event, as it increases immunity levels in the population to some extent.
Many in the public eye have been focusing on the wrong numbers. They have been suggesting that 60–80% of people would need to get infected in order to reach herd immunity. Instead, the back of the epidemic is broken at a much lower percentage of infections.
After all, we will never eradicate Covid-19. Herd protection is the goal. It may be that after 10–20% of people in a region are infected, the epidemic wave may be over for now.
As the RT (rate of transmission) gradually drops below one, cases become mostly asymptomatic upon second and third exposure. As immunity in a population wanes over time, Covid-19 will cause outbreaks of the common cold in daycares. Covid-19 will act just like the other common cold coronaviruses do. When it becomes the fifth common cold coronavirus, the Transitional Phase ends.
If we close down the world, this virus will find a way, and we will continue to face not only Covid-19 but also the negative unintended consequences of extended closures. There are no risk-free choices.
I predict it will be 2–5 years before the Transitional Phase ends and Covid-19 is merely a cause of the common cold.
How can we help the virus spread, make it weak.
Depending on the environment in which the virus lives and its mechanism of spread, it might evolve to be more benign. Imagine for a second that there are two competing strains of virus in a population. One kills off its host before it spreads, and the other is much more benign but more efficient at spreading. Over time, which version will you see more of?
If there are strains out there that kill people rapidly, we should aggressively isolate, quarantine, and contact trace those cases. Conversely, if there is a strain that only causes mild disease in people, we are better off ignoring those cases. Let asymptomatic Covid-19 spread and cause more asymptomatic infections. All things being equal, we need to be more aggressive with our control efforts for lethal or severe cases of Covid-19, and less aggressive with benign cases. If there are different strains out there, natural selection encouraged by behavior will allow the virus to evolve toward benignity.
First, understand that every human will eventually be exposed to SARS-CoV-2. Someone will sneeze or cough on you, or you will otherwise breathe it in or transfer it to your mucous membranes. It will happen. Plan on getting Covid, but later. Not now.
The end of the virus might come from left field.
My prediction: something out of left field will end the Covid pandemic. Something, someone, somewhere, has in the back of her mind will sprout and take form to decimate Covid. After all, we have botanists, astrophysicists, zoologists, and everyone in between thinking about this problem. It will be a novel idea. Something we can’t even conceive of yet will emerge and end the scourge.
In the meantime, a controlled spread (viral burn).
Controlling the rate of transmission through cultural practices such as distancing and mask use are important during the Transitional Phase. This means that we cannot reopen everything and revert entirely back to the “old normal.” Likely we will start with reduced physical distancing around those people we interact with the most. That is to say, you might give your Mom or Grandma a hug. It is hard to foresee any large crowds gathering any time soon, however. Not, at least, with some risks attached.
Masks will remain an important accoutrement for the next several years.
Moving forward we will need to continue to protect the vulnerable. We will need to sensibly and carefully allow the virus to spread, steering the virus towards a more benign form. The virus will run its course, that is a given.
As humans, we can largely determine the path and the timing of this killer on its journey to becoming the next common cold.
From Killer to Common Cold available on Amazon .
And on Amazon.ca.
Dale’s perspective and thoughts …
Thanks so much to Dr. Graham. I have followed his blog for quite some time. And David has answered my questions at every turn from the beginning of the pandemic. In March and April and May I needed to understand the virus and how things might play out.
I was concerned from very early stages. Even on February 1 (as cases were just arriving in North America) I offered … How to prepare your portfolio for the coronavirus outbreak. Of course I am more concerned with the health issues compared to any investment ramifications.
And now, I need to understand how long this might all last. I need to understand how the pandemic ends. Or at least how they pandemic might end. What are we in for?
From Killer to Common Cold is a wonderful read. It is honest and refreshing. It answers a lot of my questions. I’ve found that health experts have been afraid at times to deliver the honest goods on the virus, vaccines and the pandemic in general. Dr. Graham’s book also give us hope that we can and will get ‘to the other side’.
And remember please, be safe out there. The virus is still in that killer mode. We need to respect the virus.
Thanks for reading, we’ll see you in the comment section. I’m sure Dr. Graham would be happy to stop by the site from time to time to answer those questions.
Dale
very interesting article, thank you!
Glad you enjoyed it, thanks. Feel free to ask any questions and we’ll get Dr. Graham to drop by the site.
Dale
Hi Dale, just now ordered the book, thanks for your research on this! Invaluable!
Hi Mike thanks for that feedback. I do a lot of reading in the area. I thought I owed it to readers to share.
From Killer to Common Cold is a refreshing take on things. That said, there are certainly many unanswered questions on various theories as well as Dr. Graham will acknowledge.
Enjoy the book. I’ve heard from a few others who have ordered a copy as well. You can get a Kindle version for about $5 Canadian I believe.
Dale
I forwarded your article to several people. Dr. Graham writes in an “easy to understand” manner which is exactly what people need to read in this trying time. On a side note I lived 6 years in Scandinavia and my wife is Hungarian. She’s presently in Budapest with family and we communicate daily using Facebook Messenger. Ironic, isn’t it – never been closer in the global village and yet further apart from the neighbor next door.
Hence , for obvious reasons I follow the news in Europe and in particular the Swedish approach. (recent 3.35 minute news video from NBC News https://www.youtube.com/watch?v=K8nZOHPFdX8). Yes they had a horrific mortality rate among the elderly in the chaos of the spring wave but overall cases have plummeted even with an increase in testing and without destroying the economy. The government ran a surprise surplus in August and there is hardly a mask in sight! Despite a stricter lockdown/mask regimen it’s worse in Spain, France and the UK. Not saying the Swedes have the answer – we’re going to learn a lot as this passes – and there are a number of institutional and cultural anomalies. But we should all be looking closer at Germany, Taiwan and Sweden.
Personally I find it bizarre when people walk on the road to avoid me on the sidewalk as I’m sure we’ve all experienced to a degree. Or, the shopper in a supermarket who obviously never exercises and stuffs their cart with processed/comfort food while wearing a mask because it’s “safe”.
PS – I’m not in the pro mask or anti mask camp, rather in the discretionary use one.
Thanks Barry, we are certainly learning as we go. I only wear a mask when shopping, or with my Mom. We simply don’t entertain in large groups. We have a very small circle and we’ve been outside on the deck for any lunches or dinners.
Medical experts are learning on the fly as well. As Dr. Graham suggests we won’t know all of the answers until it’s ‘over’.
Dale
Thanks for the comments all! It is not a fun time to think about a damn virus all the time, but it is what we are all doing!
For anyone who is interested, take a look at the mid 2000s Belgian evaluation of the 1890 Russian flu. It was a worldwide killer pandemic that may have been caused by what is now the fourth or most recent coronavirus to become a common human cold, transmitted in the late 1880s from mice to cattle to humans. Looks like it took about three winter seasons for the virus to settle into cold status.
The ‘Spanish Flu’ (misnomer/it was not started in Spain at all) took 3 years I believe to run its course. Hopefully we can have a much easier go of it to the other side.
Thanks for stopping by,
Dale